The Deep Dive Nobody Asked For
Marketing Majors Remain the Scum of the Earth

I’ll be real with you folks. This season – or whatever we’re calling it – of Shucked or Unshucked is just me blurting out ‘you’re not going to believe the shit I heard at work.’
Now, someone might say ‘Evan, should you really be saying this stuff in a public forum?’ Hell, my father – a busy man I assure you – called me in the middle of the day to question my judgement in writing about such matters. But here’s the thing folks. We don’t care.
My mother used to say to me that I shouldn’t talk so much shit because eventually I would get hit. In my entire childhood I got decked in the face like one time and even then, it wasn’t over something I said – I just have a punchable face. I can’t fix that. But I can keep talking about the insanity I see other companies doing.
This week I am going to start off by giving something of value in terms of a shiny picture. This picture is an accurate landscape of the Healthcare Professional Marketing sector. How do I know it’s accurate? Well, because I made it. I also ran it past a bunch of industry professionals including the Head of Healthcare Media and Marketing Investment Banking at a very large investment bank. It’s not quite perfect but, hey, none of us are.
Here it is in all its ‘made in PowerPoint’ glory.
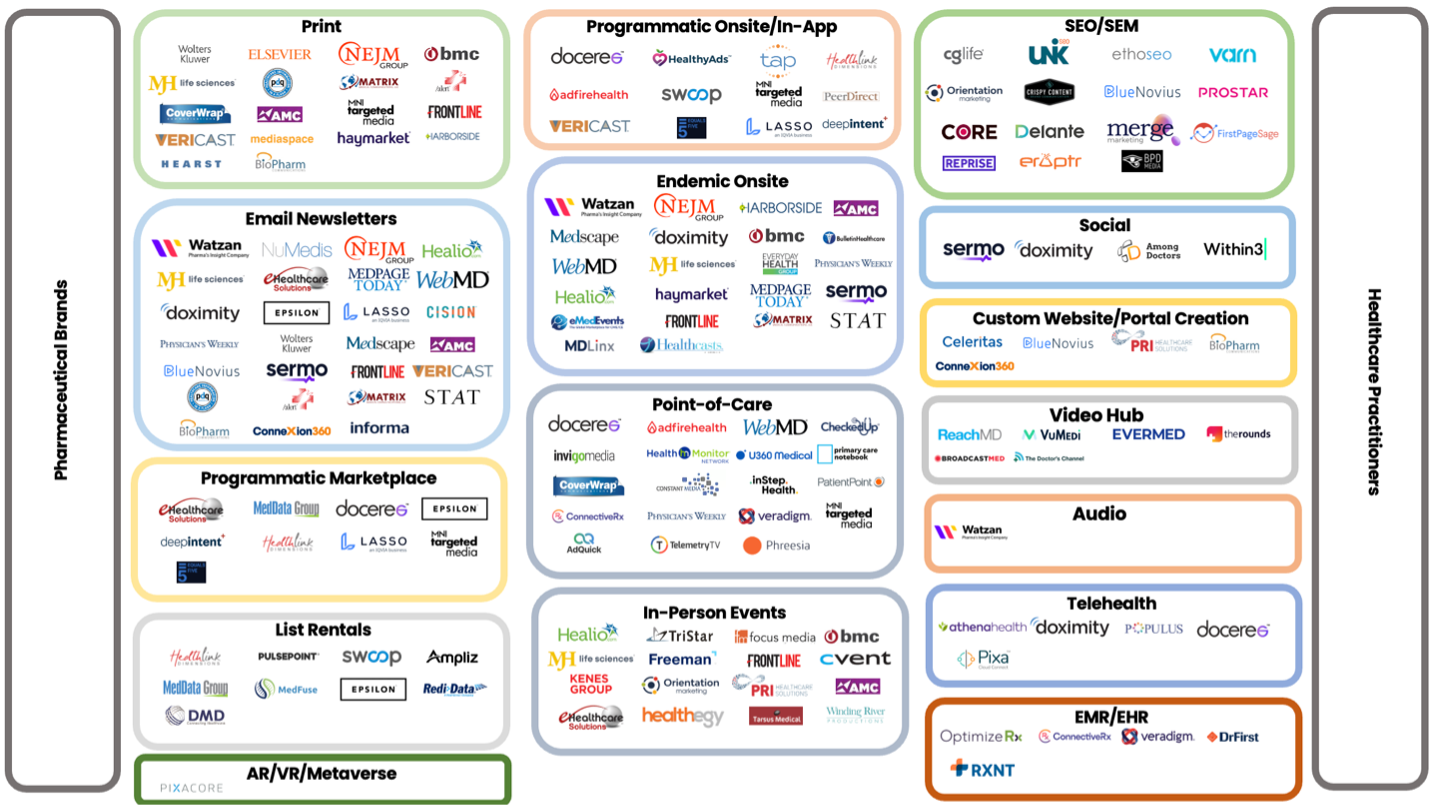
What a thing of beauty.
Fun fact, there are hundred-million-dollar media planning agencies whose entire economic value stem from their alleged monopoly on the knowledge contained in this image. Okay, that’s a lie. The value is in relationships with brands, but to brands their value is in their knowledge. My company threw this up on LinkedIn for free this week so that should tell you what I think about the value prop of those agencies.
Anyways, the point of showing this is (1) to provide readers with the semblance of value, and (2) use it as a jumping off point for the discussion today which is all about the divergence between the real and digital worlds. But first, allow me to briefly describe how healthcare marketing in the U S of A works.
Let’s say that you are Pfizer. You have drugs that you have spent years carrying through the clinical trial process. The ones that make it to market are the lucky ones. Along the way you had a number of options in your development portfolio that went to 0 due to failures. This means that a drug doesn’t just have to make back its own costs of development but also the costs of those you lost along the way. There’s a lot riding on the performance of drugs that make it to market. You can’t fuck it up. Your messaging must get out to healthcare professionals. They can’t prescribe you if they don’t know you exist.
Two posts ago I wrote about why this can’t be true. Ignore that. We are beyond the horizon of rational behaviour.
You’re Pfizer. You think it is true and, by God, that’s all that matters. In your mind, if doctors don’t know your jingle, then the shareholders will suffer. Think of the fiduciary responsibility. We’re basically dealing with something greater than ife or death. Sure, patient outcomes matter, but patients don’t attend board meetings, people.
To get your messaging out there you must hire two types of agencies. The first is the creative agency – think Don Draper. The second is the strategic agency – think every dumb fuck who majored in marketing or communications at your college. The creatives think that they are God’s gift to advertising. They ain’t. I can’t draw worth a damn so I can appreciate them.
The strategic agencies are paper pushers who ought not to have jobs. Tough; but true. They buy advertising inventory from platforms. Think of them as the ones who decide which billboard to place the giant image on. They are effectively just contracting companies.
These agencies talk about ‘strategy’ and ‘innovation’ but that’s window dressing. 95% of every media plan they come up with is copy-pasted from a competing – or completely unrelated – drug they worked with last week.
The problem is that media planners have zero understanding of the real world their clients operate in. The agencies are where people get their starts. In conversation with media planners, it has become apparent to me that few of them want to transition over to the pharmaceutical manufacturing (i.e. Pfizer) side of life [effectively the equivalent of ‘Buy Side’ in finance] due to a perception that the environment on that side is toxic. It might be. I sense a lot of backstabbing and ‘tallest midget’ competitions.
In contrast, they are quite interested in working for vendors – the folks who provide the inventory where the creative asset sits. Why? Because at the agencies they evaluate platforms RFP responses. They learn what you must put in the excel sheets to get picked for the plan. That, plus the opportunity for commissions, leads to an easy and possibly lucrative opportunity. If things dry up, they just go back to the agencies at a higher level and pay grade.
These agencies are the likes of CMI (owned by WPP), PHM (owned by Publicis), and Initiative (owned by IPG). You might say here that one shouldn’t name names when speaking in a less that positive manner, but I assure you, the folks at the agencies – if they are literate at all – lack the attention span to get this far down the post.
You want some real tea spilt? Alright, I’ll knock the cup over . One of the big agencies – I won’t say who – used to be independent (they all once were). As such they had a sister company who handled the literal contracting for media campaigns. The planning agency would buy inventory from Platform A and the sister company would handle the legal and accounting side of things. Let’s call the combination of media planning agency and contracting company ‘Bordeaux.’ Bordeaux developed a ‘preferred partner’ program.
How it worked was that the media planning agency would allocate pharma companies’ spend to platforms and if a platform hit a certain aggregate spend threshold, Bordeaux would invite them to the program. The program consisted of a ‘rebate’ which was between 5% and 10% of allocated spend paid back in cash to Bordeaux via its contracting arm. In return, the platform would get a designated representative at Bordeaux whose job it was to get them meetings with planning teams who allocate spend. The implied benefit being that more meetings meant more spend allocated. If a platform said ‘no’ to these terms, then the planning agency could – this was never said out loud – allocate 25% less spend next cycle to them in favor of a partner.
If you were the salesperson at a vendor responsible for getting money from Bordeaux, then you are fucking paying the 5% to 10% rebate because you get to book the revenue regardless and account the rebate as part of your Cost of Goods Sold or some shit. There ain’t no way you’re going to let revenue drop by a quarter because you will be fired. It should be obvious by now that this rebate is protection money.
I know of at least one of the partner vendors who has not seen an additional nickel in spend since they were ‘invited’ to the program. They’d leave, but then they’d be wiped off many a media plan.
Bordeaux was not getting a discount on vendor services for their clients. They were not in the business of spending their own money. Instead, they were playing with their clients’ funds.
Typically, a planning agency (and associated contracting arm) receives 10% of gross spend allocated from their clients. Under the ‘preferred partner’ program they would receive the 10% directly form the client plus 5% to 10% spend allocated from their vendors. Conversations with agency tells me that 90% of spend is allocated to a handful of big vendors who are all preferred partners. This means that while the pharma company thinks their agency/contracting costs are 10%, in reality, they range from 14.5% to 19% of spend.
The planning component of Bordeaux was sold to one of the global marketing mega agencies while still continuing to exclusively use the contracting arm for all their executions. Meaning that a publicly traded giant agency is being robbed blind alongside their clients. The former owners of Bordeaux – who got a shitload of money from selling to the giant agency – are the ones pocketing the ‘rebate.’ If the former planning arm of Bordeaux is allocating $500 million a year, then the contracting folks are siphoning off between $22.5 million and $45 million a year. Or at least that’s the best back of the envelop guess I can make. Wild shit in this world man. Wild shit.
Back to the main topic though. I believe journalists and investment bankers are cut from the same cloth in that they both went to school to study absolutely nothing while convincing themselves that they learned a profession. I went to a liberal arts college with a big ass journalism program and my biggest takeaway from those shit for brains was that they spoke about everything while understanding nothing. How could they? They could write a story about, I don’t know, climate change, and have zero understanding of climatic science. Or they could write about steel manufacturers without a clue regarding the factors that shape that industry.
In the same vein, investment bankers are best understood through the line in Oliver Stone’s JFK where Kevin Bacon’s character tells Kevin Costner’s that ‘you don’t know shit because you’ve never been fucked in the ass.’ How do I know this? Well, once upon a time I was getting grilled in an interview by a mid-senior IB bro in Calgary working on the Oil and Gas – I mean ‘energy’ – side of things and I said that you can frack for oil, and he decided to tell me I was a dumb fuck for a few minutes. He was under the impression that fracking only worked for natural gas. Anyway, he was wrong as shit, but still takes home mid six-figures in salary.
Think about it. You’re a bright young lacrosse player at Dartmouth. Your father is a wealth advisor with BofA Merrill Lynch, and you think you can be a big money baller. You major in economics despite it having little to no correlation with finance – a topic for another time – and intern at investment banks every summer. Upon graduation you slide into the analyst program with a Technology, Media, and Telcoms team and Bob’s your uncle.
What the actual shit do you know about that industry? Do you understand the drivers of demand? The basis of contracting? The interrelation of product, context, and audience? No. You know how to manipulate a spreadsheet and look up industry comps on your terminal. You – to reuse the reference above – ain’t ever been fucked in the ass. Yet, you will walk into a C-Suite meeting and act like the reincarnation of Walt Disney.
It ain’t just the juniors who wield delusions of grandeur, the whole chain of command on the team don’t know shit.
Media planners are the same way. They spend their days – based on conversations with them – chugging away on, admittedly, unsophisticated Excel files. They spend other people’s money in that they are just an intermediary between pharmaceutical companies and the platforms they wish to advertise on. They have, broadly speaking, never been in the trenches generating performance and sold a platform’s bona fides to someone else. There’s a complete lack of understanding of what really happens on the various platforms. Instead, they just look at KPIs that can be gamed and general sentiment around vendors. Companies perceived to be big ballers pull in cash in a manner akin to gravitation.
Allow me to provide an illuminating [but very long] example. I got hit up by the ‘Thought Leader Liaison Team’ covering rheumatology at a top-10 pharmaceutical company this week to chat about sponsorship opportunities on one of my company’s platforms. It was a great call. The folks from pharma had unique roles in that while they were paid out of the marketing budget their roles were to be the ‘boots on the ground’ talking with the biggest rheumatologists in the land about what they liked, were up to, and thought was cool. That’s how our platform came up. Big win for us.
On the call, the TLL team – as they called themselves – let me in on a little secret. They were fresh off an internal conference where they saw a bunch of data about the platforms that their ‘customers’ (i.e., rheumatologists) use. You want to guess what the number one platform rheumatologists in the United States trust and read daily is? I’ll give you a hint, it ain’t listed in the landscape above. It’s a website based on simple WordPress code.
This website is run by a recognized physician named [redacted]. Let’s call him Dr Bob. He does stories, videos, podcasts, and email newsletters. He is a god damn baller in the rheumatology space. Dr Bob is the fucking man. You wish you were Dr Bob. I wish I was Dr Bob. Dr Bob probably has fourteen Porsches and a mansion in Grenada. Dr Bob is the Toto Wolff of rheumatology. He exudes excellence and sweats Benjamins.
Except here’s the thing. He does not get the most money when it comes to pharmaceutical advertising in rheumatology.
The following image reflects internal estimates I made regarding total conference spend by the biggest brands in rheumatology on in-person efforts at the annual general meeting of the American College of Rheumatology in 2022:
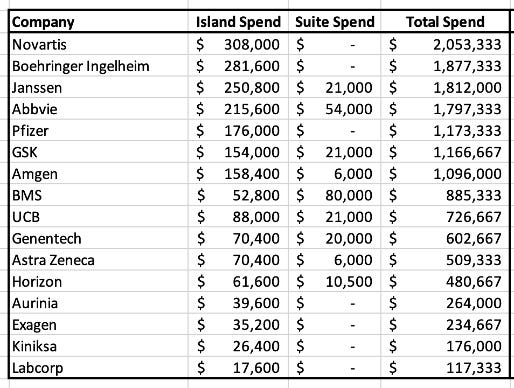
I’m not going to get into the methodology because I don’t have to, but it passed the industry sniff test.
Of the brands who spent over $1 million at the conference, it is safe to say, spend somewhere in the neighbourhood of $10 million in digital advertising per year. The large platforms in healthcare professional marketing do not get out of bed in the morning for less than $500,000 in program spend. This I know from industry conversations.
For context, I’m looking at a particular vendor’s rack rate package and to simply include assets in a single email newsletter wave to 4,000 US-based healthcare practitioners (a bit below the size of the rheumatology population) costs $17,000. If you send out a wave a week that’s $884,000 just for one tactic on one platform. I’m not saying that a given brand is going to buy a full year of newsletter inventory, but all brands in aggregate within a specialty will likely buy 52 weeks’ worth of stuff from the vendor. Note that we’re talking about $884,000 per specialty or indication so you could have dozens of indication-specific email newsletters going out.
By contrast, Dr Bob’s site has limited inventory. The good doctor does not have time to create content and distribute it in a relatively infinite number of indications. He’s busy being a Greek god of thought leadership. Additionally, the site is not exactly sophisticated. Without knowing too much about their operations I assume they do limited advertising consisting of banner assets. The site might do like $2.5 million a year. It could also do something in the low six-figures. We don’t know. My guess is that $1 million in revenue might be the ceiling because there aren’t many – if any – banner assets existing on the platform. Additional funds come from pharma companies sponsoring content in the sense of ‘here’s twenty grand just to talk about a condition and not mention our offering by name.’
Based on industry conversations I can say that the site gives Dr Bob a thought leader status that can – without getting into the details – be extremely lucrative [and rightfully so]. But this is not about our boy Bob. It’s about the fact that if there is, let’s say, $100 million in digital advertising being spent in rheumatology each year (probably even higher in all honesty) the #1 rheumatologist-visited and trusted platform is not getting the bulk, or even the most, spend.
As mentioned above, 90% of spend goes to a hand full of big platforms. So, $90 million goes their way, Dr Bob picks up like $1 million and everyone else throws hands over the remaining $9 million. This should seem absolutely bananas to any rational person.
Let’s say there are 5,000 rheumatologists in the United States. Furthermore, let’s say that in total, Bobby boy’s site gets on an average 1 visit per rheumatologist per day (lumping in folks who don’t use the site in the average calculation). That’s 5,000 visits a day and 150,000 a month.
This figure isn’t crazy. I don’t know what their numbers are exactly. But I’m not just building castles out of clouds.
In conversations with folks this number seems to be at least ballpark reasonable. The result is that the number one platform, as reported by rheumatologists, might be getting 150,000 relevant visits a month. This ought to be the ceiling in the rheumatology market. We are ignoring multiple page view sessions here because all the numbers are made up anyway.
If the big platforms are getting $90 million a year in rheumatology that’s $7.5 million a month. Brands do not pay based on a per-visit model. They pay based on shit like impressions, clicks, and video views. But let’s say that – all else being equal – aggregate brand spend is correlated with audience size and activity (i.e. number of visits per month). If Dr Bob’s site has 150,000 and makes [estimating] $83,000 a month, then you would have to have over 13 million ‘visits’ across the big platforms. What does this entail?
Let’s say that the average rheumatologist works 8 hours a day. Additionally, let’s say that the average patient visit is 15 minutes long. Furthermore, let’s say that during these 15 minutes the rheumatologist ‘visits’ a platform for information or some shit (obviously this is a ridiculous assumption but stick with me). At 5,000 rheumatologists in the US, times 32 appointments a day, multiplied by 30 days a month, you get 4.8 million visits per month.
But how often does a doctor look at a doctor-focused digital platform? In the hypothetical above we assumed that they were looking 32 times a day. Who the fuck looks at work-related content four times an hour? You think an engineer is looking up recent advances in structural steel every 15 minutes? No. They’re busy working. So, let’s say maybe they look 10 times a day and even that seems hella aggressive. That leaves you with 1.5 million visits. Again though, the most visited platform is pulling like 150,000 visits a month.
Are there 9 other platforms pulling numbers those kinds of numbers? No, there ain’t, because docs are too busy to stare at their phones all day. Yet, planning agencies are allocating north of $7 million a month to the big platforms. If you assume that each visit generates 3 impressions (a contractual unit) that’s 4.5 million impressions a month for a total CPM (cost per thousand impressions) of $1,555. For reference, an average consumer CPM is $0.5 to $4. There’s a lot of money here relative to the effort and work required.
Let’s think about what we have here. The #1 site for rheumatologists in the US is pulling in something like $1 million of a total pie of $100 million. Meanwhile, around ten ‘big’ platforms are likely pulling in $90 million. Does that make sense to you? Because it makes none to me. Except until you realize that media planners don’t know shit.
Here’s my theory of what happens. If you are a 22-year-old recent graduate of Temple University and get hired as an associate media planner at one of the agencies, you effectively know nothing. However, you have all these responses to RFPs come your way. You copy information into excel files and based on vibes and the numbers in the cells, you and your bosses select platforms for the placement of advertising units. So long as the KPIs are met and your ad auditing platform does scream FRAUD at you, it’s a success. At no time along the way do you talk to a physician about what platforms they use and value. That’s where you rely on industry surveys.
These surveys can be very valid. Let’s say that in rheumatology they state that Dr Bob’s is number one in physician recognition with the big platforms following behind it. The problem is that Dr Bob’s site does not have all that much inventory. As mentioned, when I go there, I don’t see banners. Maybe it’s set up so that you have to be signed in and validated as a physician in order to see ads (a normal thing in the industry) but even then, it’s just one site and one mailing list. The site takes its $1 million a year and then says, ‘fuck off we’re full.’ But you have a client who is paying you to put their assets somewhere.
The big platforms step up to the plate with their hand out and say ‘we’ll take that off your hands’ and despite not being as trusted or as visited as Dr Bob’s site they sell as much inventory as they can. Along the way they juice their numbers to make it seem like brands are getting lights out performance. What does that mean though?
All the money in pharma comes from specialists. Your run of the primary care physician can’t really do all that much in terms of pushing dollars via prescriptions. At least not from a profit point-of-view. Meanwhile, there are like 15 surgeons in the United States who can perform ophthalmological gene therapy procedures that run $80,000 to $100,000 a pop. When an advertising platform is paid based on the number of actions that occur on it then engaging just those 15 would be a great way to lose money. No one is going to pay millions to hit up two dozen schmucks. So, what’s a platform to do? Great question.
Platforms make their bones by engaging non-specialists. If you are a family doctor and you see a wide swath of patients with varying ailments every day you are naturally going to be outside of your area of expertise on a regular basis. As a result, you will go a digging for information to either address an immediate concern or stay generally up to date across specialties. In contrast, specialists know infinitely more about the conditions they handle daily than the folks who put together content on physician-focused platforms.
If you’re a lung cancer specialist, you will not spend much time educating yourself on platforms. You know the offering landscape and the emerging treatment options because you go to the relevant sessions at your regularly scheduled conferences. There also aren’t that many treatment options. If you’re a rheumatologist with patients suffering from uncontrolled gout, you’re going to prescribe them Krystexxa because there ain’t nothing else out there.
The fact of the matter is that you have brands who, in theory, are looking to engage specialists or specialist-adjacent physicians who could refer patients to specialists. At the same time, platforms have a shit ton of non-specialists. Smash these two things together and you have a clear disconnect that doesn’t work. Yet money keeps flowing and KPIs are met. So, what gives?
The answer lies with the planning agencies. The planners ain’t doctors. Furthermore, they never talk to the docs. Instead, they have a client looking to spend a lot of money and platforms willing to take as much of it off their hands as possible. So, what happens is that the brands create target lists of physicians that run into the thousands when they only need to hit up a couple hundred at most. The list includes specialists and non-specialists. The platforms go ‘we can hit 90% of the target audience’ and off to the races they go.
Performance relative to the program comes from the non-specialists while the overall platform traffic numbers are driven by family physicians. The problem, as you can probably guess, is that neither of the active groups are who the brands want to reach. It’s like if a brand was selling soccer cleats but instead of advertising to only soccer players, they went to everyone who has feet and counted all activity as if it were from soccer players. You’re effectively paying to engage people who couldn’t care less while pretending that you only reached the most likely customer.
What’s something constructive we can say? Well, a useful takeaway here is that brands ought to be focusing on what I call quality platforms. The definition of quality being – a place where relevant healthcare practitioners are active on a regular basis. In this scenario Dr Bob’s site is the pinnacle of quality vis-à-vis rheumatology platforms. But he lacks the inventory to satisfy everyone. What happens is a race for lower quality inventory. Except that the price elasticity of quality is inverted just below the top tier. Lesser quality platforms charge far more than Dr Bob does just for the privilege of letting you buy a fuck ton of inventory.
Imagine that it’s 2020 and we’re all pretty sure that we’re going to die. I studied plagues a bit in college and my thought in March 2020 was ‘oh drink up boys because we fucked.’ If you’re the government of a rich country, you wanted to buy a butt load of high-quality medical PPE. Except there was only so much that was out there, and high quality takes time to make. The highest quality got bought up at let’s say X dollars in five minutes. Then everyone panicked and starting spending like drunken sailors for anything. The next tier folks capable of providing a ton of shit charged through the nose because countries like France needed masks – for example – by the billions. Macron was happy to drop 100 X so long as he got something. This is what happens in pharma marketing. Good money chases bad quality for the sake of just getting assets in market.
The company I work for is in the early stages of marketing a platform that – we believe – solves the quality/inventory trade-off so feel free to send me your money Big Pharma. But ultimately, contrary to the statement above, there is no constructive takeaway here. Well, other than, ‘give me your money folks because at least I’m honest,’ but that’s not really appropriate, eh?
The title of this piece reflects its deep dive nature. It’s more of a ‘telling you how shit works’ post than an essay with a thesis other than ‘look how fucked up this shit is.’ If you’ve made it this far you should walk out with at least this takeaway – doctors don’t use doctor focused platforms 1/10th as much as the platforms say they do and you should pay through the nose for quality instead of inventory because the inventory you buy is shit.